continued from the above:

So I’m very, very happy to say that the primary endpoint, the median overall survival in newly diagnosed glioblastoma patients reached statistical significance, as did the secondary endpoint… that is the patients with the recurrent disease who had dendritic cell therapy had improved survival.
The safety profile was excellent. There was 2,193 doses of DCVax administered, only five adverse events were reported, and no significant and immune reaction.
Share price: $0.925
Overall Results - 5 Key Data Points Slide
 So the important landmarks are
So the important landmarks are that the median overall survival of patients with newly diagnosed glioblastoma was
19.3 months from randomization and 22.4 months from surgery. And this is versus 16.5 months that you would expect normally and we’re seeing in the randomized controls. Methylation of MGMT, which is a good prognostic marker for these patients,
showed a very enhanced survival of 30.2 months from randomization versus the normal expected 21.3 months. And what was extremely impressive is that the survival at five years in these patients is 13% versus 5.7%. When we look at the recurrent glioblastoma, the median overall survival was
extremely impressive as showing a 13.2 for median overall survival as opposed to the 7.8 expected median overall survival. And even here we see a survival tail at 24 months… we see 20% of patients alive. And at 30 months, 11%, which is much better than you would expect for these patients.
Share price: $0.92
Innovation Slide

So there’s been innovation in this trial, and this had to come about because of the cross over design that was required in this.
But this is the first phase three trial of a systemic treatment in seventeen years to show significant extension of median overall survival in newly diagnosed glioblastoma, and the first phase three trial of any treatment in twenty seven years to show a significant extension of median overall survival in recurrent glioblastoma. These are extremely important statements, and are very, very exciting, and really important for this patient group.
And what is particularly important is that this phase three trial shows meaningful increases in long-term survival, both in newly diagnosed and recurrent glioblastoma.
(and the share price drops another $0.03)
Share price: $0.89
Broader Perspective Slide

What’s interesting with this particular treatment is it has little or no toxicity. And it really is suitable for combination with a wide range of other treatments which people can spend a lot of time thinking about: checkpoint inhibitors, oncolytic viruses, cytokines, chemotherapy, etc. And what’s also really exciting is wit this particular technology is that when the patient recurs, and they have further surgery, you can make a new batch with this treatment, and so the targets, so this tumor, evades treatments because it changes. But you can actually just change the treatment with the tumor. And potentially, this works in glioblastoma, so it can actually work in other tumor types. So this is really a very, very exciting technology.
Share price: $0.86
Future Opportunities for Combination Therapies

This slide just looks at how it can be combined, and what people can do with it in the future.
Share price: $0.86
Newly Diagnosed GBM
 Overall Survival in Newly Diagnosed GBM Slide
Overall Survival in Newly Diagnosed GBM Slide 
So this shows the overall survival Kaplan Meier curve in the newly diagnosed patients and you can see this is very, very favorable. And you can see very clearly that there’s no cross over… and you can see the long-term survival, which is very impressive for this group of patients.
Share price: $0.878450
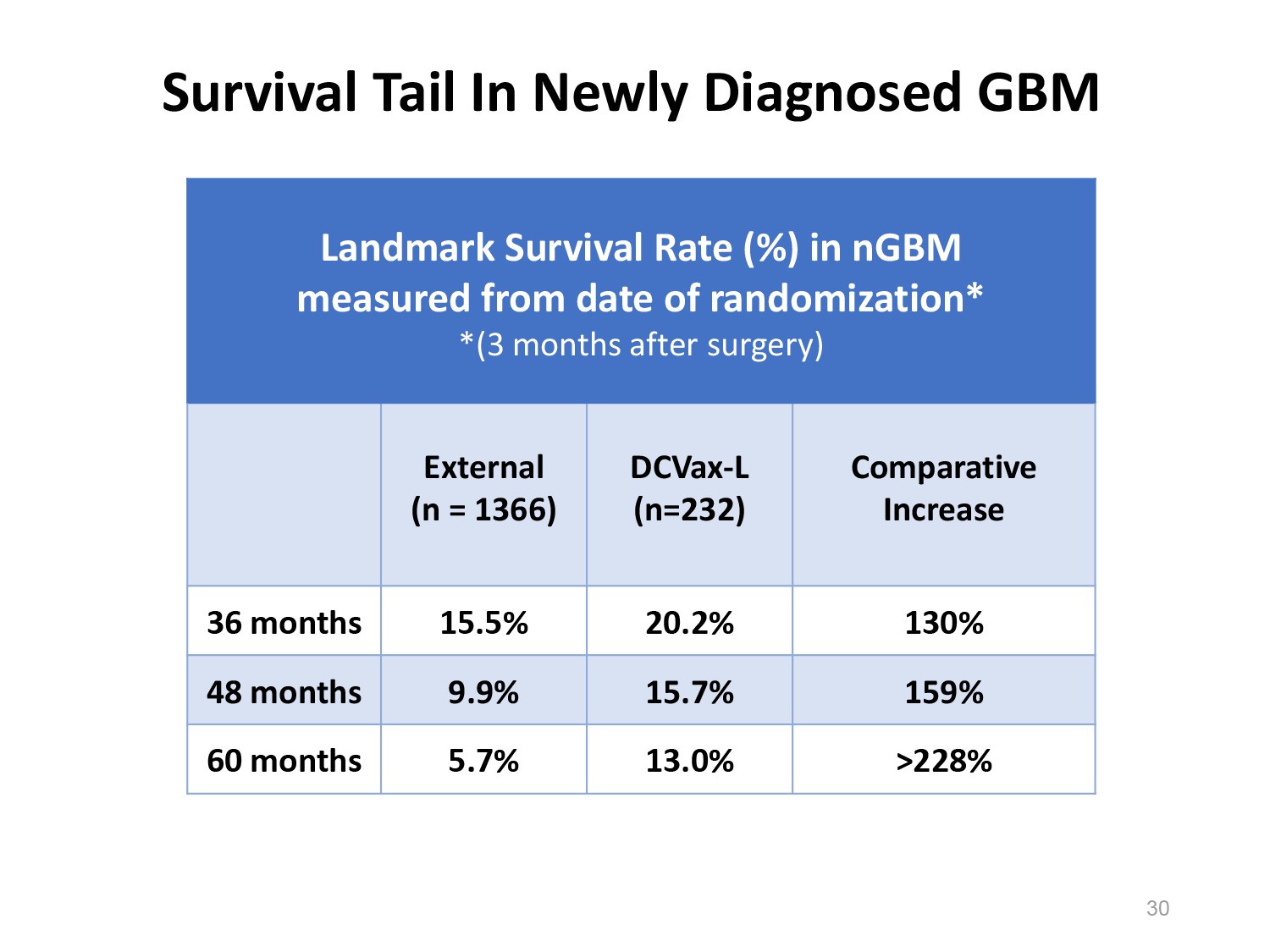
Survival Tail in Newly Diagnosed GBM Slide

So these are the important landmark survival rates in the newly diagnosed patients. So at 36 months, you have a 20% survival, 48 months, 15%, and 60 months, five years,
you have a 13% survival as compared with what you’d expect normally of around 5%.
Share price: $0.899
Pre-Defined Sub-Groups: Summary Slide

And when we look at the sub-group analysis, you can see here that actually in every sub-group analysis, there’s a favorable outcome. So when you look at age and residual disease, and when you look at this particular marker which is a gene called MGMT, that when it’s methylated, the patients have a favorable outcome.
But you can see it’s much more favorable when they have this treatment.
Share price: $0.86
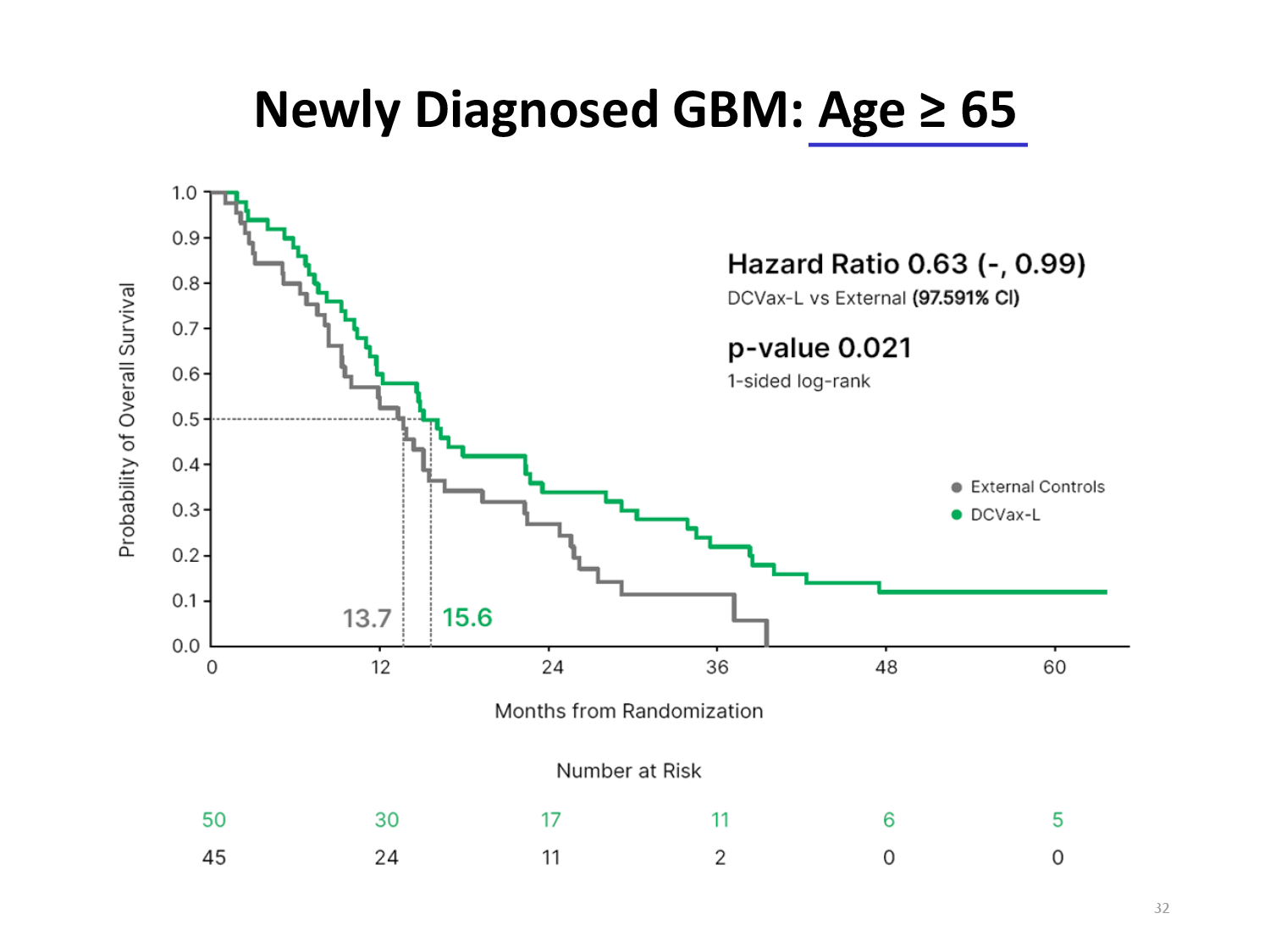
Newly Diagnosed GBM: Age Greater Than or Equal to 65 Slide

This is looking at newly diagnosed glioblastoma, and this morning, this is the first time that I’ve seen this slide.
And I am really very, very intrigued, I’m very excited. This shows that this technology which is extraordinarily well-tolerated, is showing an increase in survival in patients over 65.
And you’re showing long-term survival in this patient group.
Note: and the share price drops another $0.45 cents per share on that news.
Share price: $0.8151
Newly Diagnosed GBM: Age < 65 Slide

And when we look at the under 65s, these people have a better prognosis generally, but actually, with this technology,
it’s actually improved further.
Share price: $0.8103
Newly Diagnosed GBM: Significant Residual Disease Slide

And then when you look at this very poor prognostic factor of significant residual disease, this is really impressive. You’re seeing that this technology,
this dendritic cell vaccine, is impacting on this patient group in a way that I would not have predicted. So it’s really very, very interesting.
Share price: $0.8011
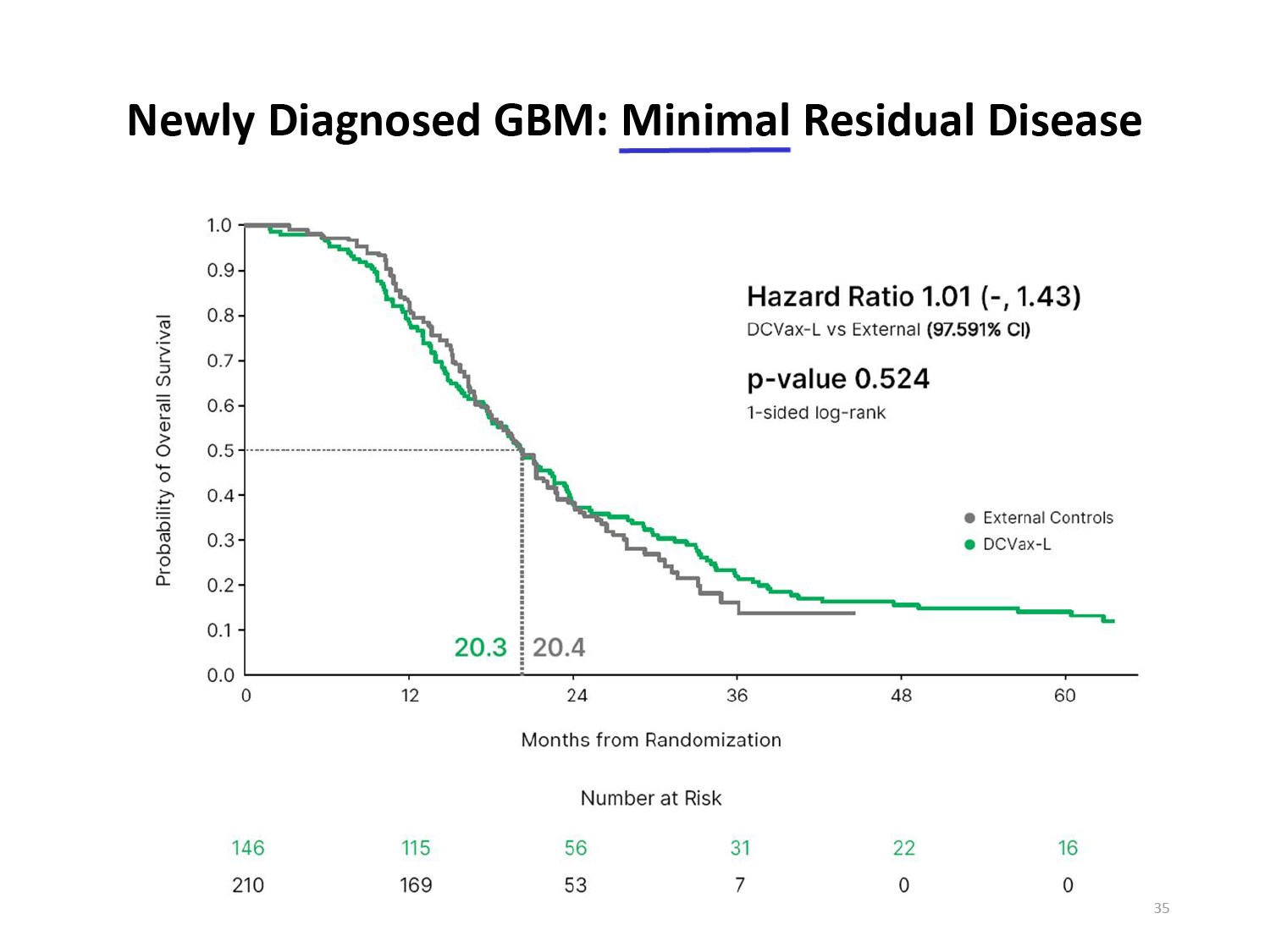
Newly Diagnosed GBM: Minimal Residual Disease Slide

Now when you look at the patients with minimal residual disease,
there’s also an advantage in survival there.
Share price: $0.80
Newly Diagnosed GBM: MGMT Methylated Slide

And this is the methylated group. This is people with the favorable gene configuration of methylated promoter region of MGMT.
And when you look at the five year survival in this group, it starts to look really interesting. And really, there is nothing that could have predicted this survival in this patient group. And it’s so impressive.
(Note: and the share price drops another $0.04 per share!)
Share price: $0.761
Newly Diagnosed GBM: MGMT UnMethylated Slide

And this is the patients that have a very poor prognostic marker of unmethylated promotor region of MGMT. And even they have a survival advantage, even though it’s smaller.
Share price: $0.75
Recurrent GBM Slide

Then we come to the recurrent glioblastoma where really, very little makes an impact. And I would not have anticipated that these patients would have had an impact with dendritic cell therapy.
Share price: $0.722
Overall Survival in Recurrent GBM Slide

But actually, when we look at the overall survival in recurrent glioblastoma, you can see the survival. And if you treat this condition,
you’ll see that that is a very favorable survival curve for recurrent glioblastoma.
We’re seeing 13.2 months median overall survival, and we’re seeing a tail, a survival tail, that goes out to five years.
(Note: hello, the share price drops another $0.02)
Share price: $0.70
Survival Tail in Recurrent GBM Slide

And here we can see the landmark data… so in recurrent glioblastoma, six months is a landmark because people aren’t expected to make it six months. But with DCVax-L, their survival is 90%. And at 24 months, 20% survival,
which is really very, very impressive. And at 30 months, we’re seeing 11% survival.
Share price: $0.72
Why/How Does DCVax-L Work Slide

So dendritic cell therapy - how does it work?
Share price: $0.744
Key Characteristics of DCVax-L Slide

I think that this audience is probably more familiar with that than a brain tumor audience. It uses the master cells of the immune system: dendritic cells, to mobilize multiple elements within the immune system. The technology that’s used in manufacture of DCVax-L is fully personalized, and it inherently targets antigens which are actually on the patient’s tumor, and fits the patient’s version of the cancer. So it really is a personalized vaccine.
And unlike other technologies, it uses all of the tumor antigens, not just some manufactured peptides, and it makes difficult for tumors to mutate around the antigens that have been targeted.
Share price: $0.7549
Larger Multiplier: Dendritic Cell Activates Hundreds of T Cells, Diverse T Cells & Other Immune Cells Slide

So this just shows a slide on how the dendritic cell, autologous dendritic cells work, and how they multiply and activate these T-cells.
Share price: $0.75
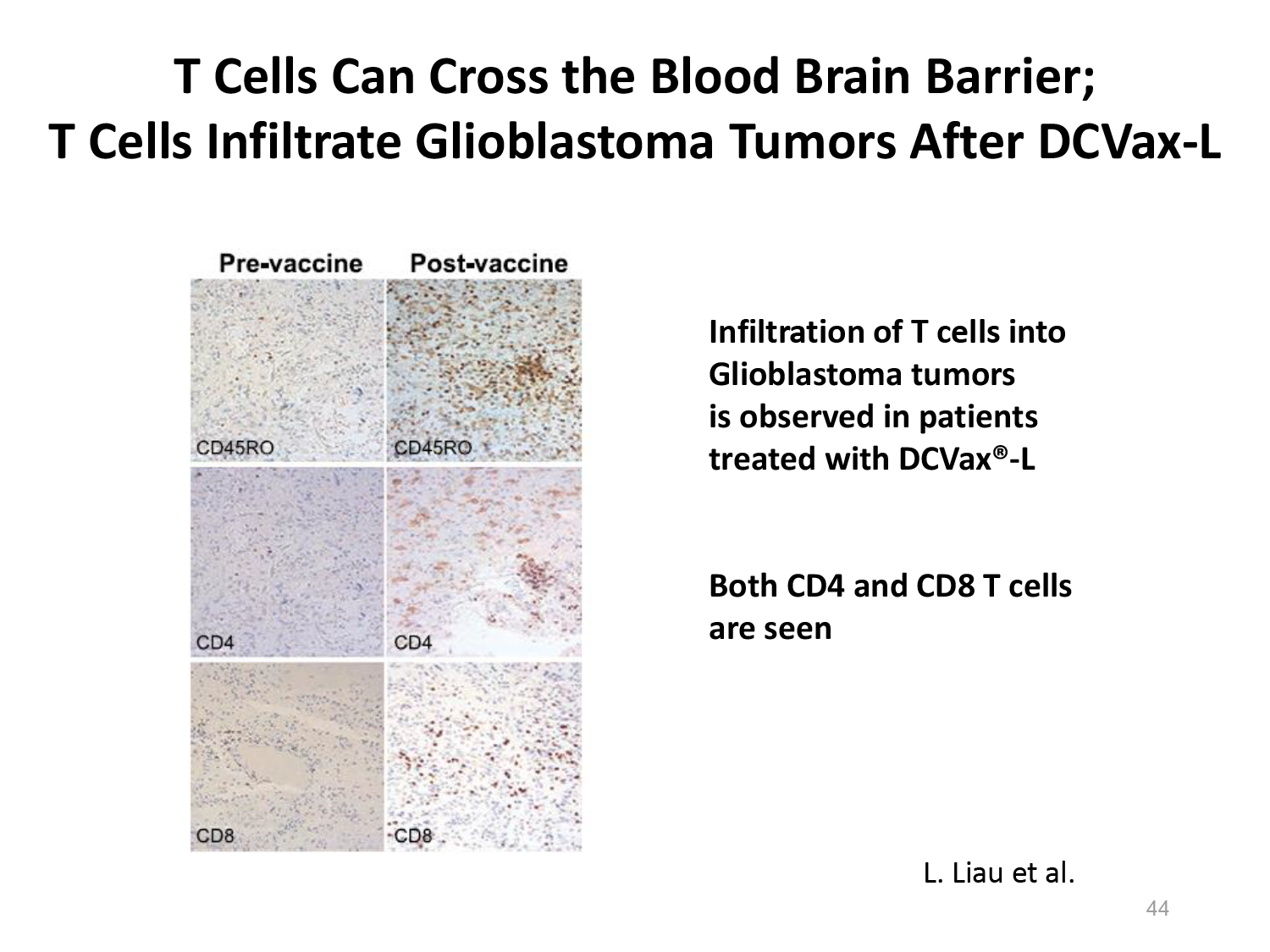
T cells Can Cross the Blood Brain Barrier; T cells Infiltrate Glioblastoma Tumors After DCVax-L Slide

And this is just a slide, so… there’s actually lot of evidence that T-cells cross the blood brain barrier - both in animal models, and also now in humans. And this is some unpublished data from Dr. Liau which shows infiltration of T-cells into glioblastoma tumors in patients who were treated with DCVax-L.
Share price: $0.76995
Conclusions (1) Slide

So in conclusion, this shows the completion of a large phase three trial including 331 patients. It was really a mammoth effort over many years, and
I was very, very honored to be part of that journey with all my co-investigators, and with
Northwest Bio. There was 94 sites, 70 clinical investigators, four countries… and I think it’s very exciting that
we’re seeing practice changing results, not only in newly diagnosed glioblastoma, but also in recurrent glioblastoma.
I can say from personal experience that this vaccine is easily administered, and has a very, very favorable side effect profile.
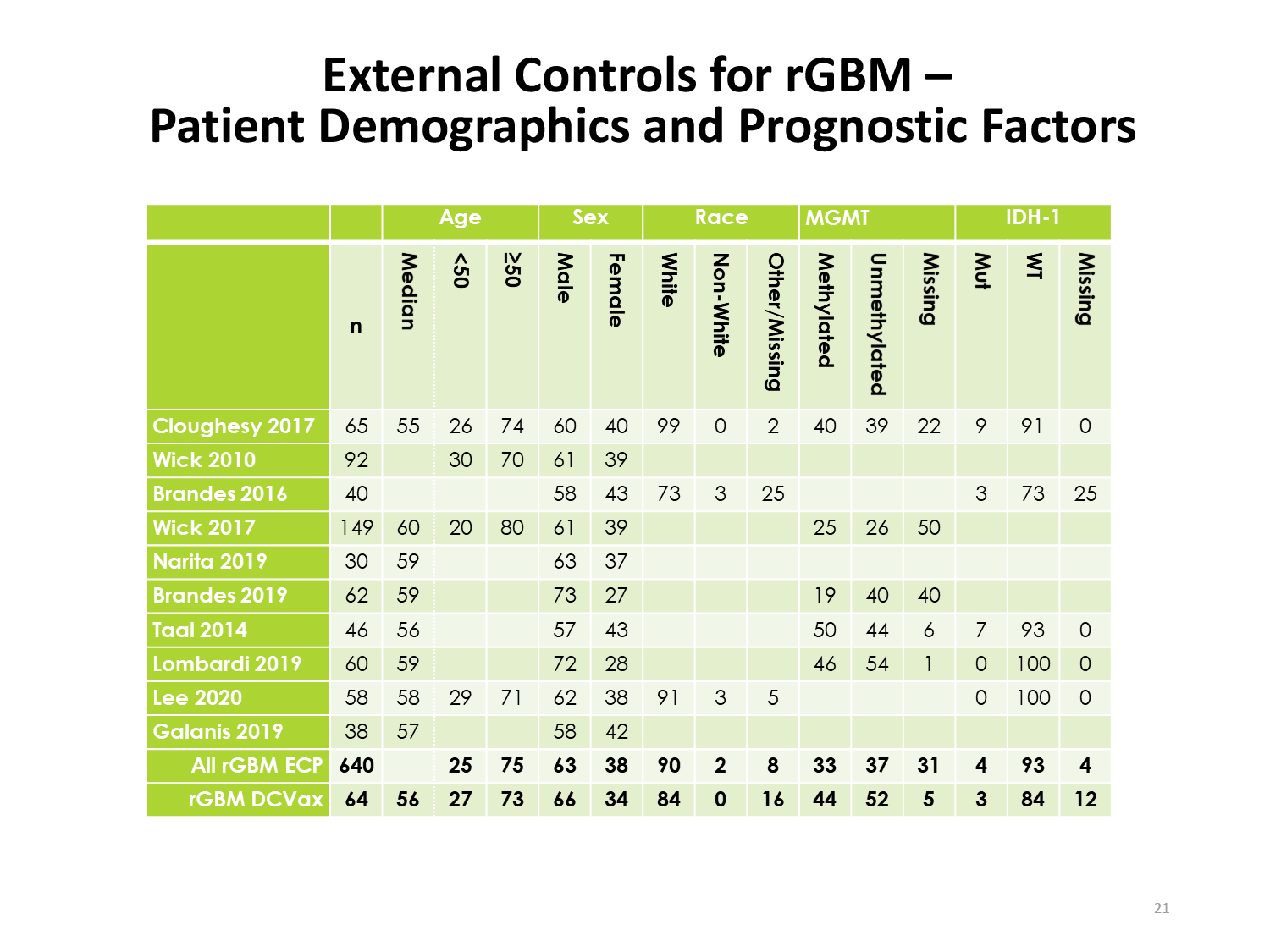
The use of these external, contemporaneous clinical trials is innovative, and I think it’s been really important for this particular trial, because the patients in this study at recurrence had the vaccine, and the vaccine was effective. Actually, we need these external controls.
And what’s particularly significant is that there is a significant percentage of long-term survivors. And that’s consistent with immune memory effect by the T-cells. And this really can change the natural history of glioblastoma, and I don’t think we’ve really seen that here with any other treatment.
Conclusions (2) Slide

And we’re still looking at the data on this, and
I’d only seen some of this data this morning, and I’m really quote overwhelmed by it. That we’re seeing sub-populations that I wouldn’t have anticipated to see benefit. We’re seeing old patients, patients with residual disease… doing really well with this treatment,
which is really quite dramatic.
So this treatment is really feasible, because there’s no side effect profile, or very little side effect profile, and it really is possible for this to be rolled out as a treatment around the world. And thinking about how we can use it going forward… of course, we need to think about combination treatments, and we also need to think about what, how is this changing the immune microenvironment. More work is ongoing in that, and I think it’s a very exciting area of research.
Share price: $0.79995
Summary Slide

So in summary,
I can say that patients treated with DCVax-L showed a clinically meaningful and statistically significant extension of survival in both newly diagnosed and recurrent glioblastoma. Patients have an excellent safety profile and it’s really noteworthy to see these long tails of survival.
Share price: $0.811
SummaryAcknowledgements Slide

So I’d like to thank Linda Liau for giving me the opportunity to speak today, and I’m sorry that she was unwell to miss the talk, and I know that that will be a regret for her. And also to Dr. Robert Prins, who led the study from UCLA, and to my college, Professor Ashkan, at Kings College, and to all my colleagues who are investigators, and sub-investigators, and the trial steering committee (Professor Steven Brem - UPenn, Dr. Jian Campaign, Washing U, now Mayo Clinic, Dr. Fabio Iwamoto, Columbia University, and Dr. John Trusheim, Allina Health), and of course, to all the patients and their families who participated in this landmark study.
So I’d be very happy to answer some questions now, if anybody has any.
Q&A
Session Host - George Zavoio:
Well, thank you very much for a very, very interesting presentation. Congratulations on the survival benefits that you’ve seen in these patients. The floor’s now open for questions. We’re going to do about five minutes of questions, so… David?
David Reardon:
Hey Paul, it’s Dave Reardon from Boston.
Congratulations, a really wonderful study and great work. Did you find out about the IDH status of the patients who enrolled, what about steroid use for patients who enrolled, and why you might anticipate the unmethylated patients didn’t benefit? Was there maybe some synergy with chemotherapy that caused immunogenic cell death and enhanced antigen priming or some other reason why the patients who got chemo seemed to have a preferential benefit?
Dr. Mulholland:
Yeah, it’s really quite interesting. So the IDH status… of course, it wasn’t stratified for them because we didn’t have this IDH status at that time, but we do have the have the data on the steroid use. Steroids were used and permitted in the study, but they were limited to less than four milligrams. And then the question about the unmethylated patients… it really is interesting, and you’re quite right, that’s the conclusion that we’ve drawn… that there must be some synergy with the temozolomide where the temozolomide is active in these patients.
But, yeah, it’s interesting, and I’m not sure we can explain all the results, but it’s great to see them.
Session Host - George Zavoio:
David, Marnix Bosch from Northwest Bio would like to add something to that answer.
Marnix Bosch:
Thanks, and thanks for the question.
Actually, the number of IDH mutations was, I think, seven patients out of 331, which is lower than what you saw in the comparator groups.
(Note: the average percentage is 7 to 10%… so to have been even comparable, there would have been 23 to 31 patients ... and of course, there were less IDH mutated in the DCVax-L trial.)
So that doesn’t contribute to the results that we’re seeing.
The question about methylation versus unmethylation I think is very interesting, and sort of raises speculation as to how this treatment can best be combined with other treatments. An answer to that would be more speculative to that than anything else, and right now, it’s an interesting observation… I agree with you.
Share price: $0.83
David Reardon:
The study, as you indicated Paul,
really is quite innovative and sets a potential precedent for the use of these external control groups which many studies are now incorporating, to a degree, and will make randomized trials much more easy to do, much more readily doable, but… was there any kind of validation, I wonder, within this study, of patients who enrolled to show a survival benefit of the, outside of the external controls, because usually when we bring external controls in, there’s kind of an internal group of controls where there’s a validation, and then you expand that with the externals. Here, the control group is really consisting exclusively of the external controls. So for example, for patients who progressed, who got vaccine versus those who didn’t, was there survival benefit for the patients before cross over, or amongst the patients who didn’t cross over, maybe? Was any kind of… could you tease out anything from the internal control patients to support the results for the external control validation? Do you mind making that clear at all?
Paul Mulholland:
I think maybe Marnix, if you could comment on that.
Marnix Bosch:
There was quite a bit of validation of the external control arm controls, actually. One thing we did is we compared the treatment arm of all the trials that were selected for comparison against external controls, and asked the question whether the results compared to external controls in those trials were consistent the ones that were originally observed for studies. As you know, almost all of those studies, except one, the Stupp trial for the Optune device, were negative. And if you compared the treatment arms of those studies to the external controls, you get exactly the same result. So I think that’s a very important comparison. Another thing, we did several sensitivity analyses. We did what’s called an
MAIC (Matched Adjusted Indirect Comparison) where you even more closely than… so the populations were already quite well matched in terms of prognostic factor and demographics, which are never perfectly matched, but you can then go back, and more and better match your population to the control population which reduces statistical power. But if you do that, then you maintain a significant positive outcome.
Then there was another series of sensitivity analyses that we did… just to give you an example… one was called
“leave one out” analyses, where subsequently, you move one study from the external control cohort and again, the results were completely identical.
Then there was one other test that we did, because two of the trials did not specify clearly to the comparator trials in newly diagnosed GBM… the two Gilbert trials… did not specify specifically whether they removed patients with recurrent disease, and from eligibility, recurrent disease, early recurrence at both chemo/radiation. So we removed those two from the comparison as another sensitivity analysis… that also did not change the result.
So that does give you a sense of the rigor that we went through to validate these comparisons.
Thanks for that question.
Share price: $0.7868
Paul Mulholland:
Thank you Marnix.
Someone:
Hi, really interesting to see you’ve got data from external controls here. Question I have is I see there were about 1400 patients in your external control. Did you find that you had non-missing data from all the 1400 patients which is what the FDA generally requires?
Share price: $0.808
Marnix Bosch:
We were, of course, dependent upon what was published. And so you extract individual patient… you reconstruct individual patient data form the published Kaplain Meier plots. Now fortunately, those trials were described in very great detail, both including demographics, etc. I think in terms of the quality of the comparison cohort, it really couldn’t have been any better, which was really the result of the other studies that were really well executed.
Same Someone:
So this was mostly a comparison to a historical control, rather than individual patient by patient matching using propensity scoring for statistical analysis.
Marnix Bosch:
Well, there was not propensity scoring because for that you need actual patient data and those have not been made available for comparison. I think that’s something that we should address in the future, that actually should be done. But these trials can be even more rigorous than they already were. I wouldn’t call them “historical” controls because they were from contemporaneous trials. They were conducted at the same time, roughly, and comparable institutions of the same quality with very much the same parameters.
So that, I think, underscores the validity of this approach.
Share price: $0.8101
Same Someone:
Thank you.
Another Person:
Clarifying question about site of vaccination. This is sub-dermal, or intra-dermal vaccination right, not intra-tumoral?
Marnix Bosch:
Intradermal.
Same Another Person:
Okay. And do you, there’s potential, because the site of vaccination is very important on, whether it be oncolytic viruses or dendritic cell vaccines… what’s your thought on what your (garbled) would be?
Marnix Bosch:
Yeah… we had a lot of talk about that. And we put this in the upper arm, sort of thinking in a very simplistic way that the closer you put it to the tumor, the more effective it will be (laughing). But often I say you can probably put it in the big toe and it won’t make any difference, as long as the dendritic cells can get to a lymphoid organ, probably a lymph node, right? It can interact with T-cells. Those T-cells travel anywhere through the body, and actually make it to the tumor site, no matter where they are induced.
Same Another Person:
We had talks about intratumoral injections for the vaccines, and that looks like a palatable pathway.
Marnix Bosch:
That would be a completely different presentation.
Share price: $0.7901
Session Host - George Zavoio:
We have one more limited… one more… from (garbled)? Lemme do that first… give virtual attendees a chance.
The most popular question of our virtual audience is what is the process for FDA approval now?
Marnix Bosch:
We really can’t speak to that. It will be no different than for any other treatment.
Session Host - George Zavoio:
One more question.
Yet Another Person (Drr. Stephen Brem?):
Yeah, I wanted to answer David’s (Reardon) question… and congratulate Paul Mulholland, the Northwest Bio team. Without being self-congratulatory… full disclosure… I’m one of the seventy authors, and we’ve been waiting for an advance like this for a long time.
David, in addition to the external controls and the numbers, we have some unpublished data from (garbled Penn?) and Dr. Mulholland’s team has been looking at radiological markers, and we’ll present that in June. That will obviously add to the story in terms of using each patient as a control, and having another dimension of efficacy. Thank you.
Share price: $0.754
Session Host - George Zavoio:
Alright… thank you very much. We went a little bit over on time, but I think that this is an important presentation that generated very interesting questions.
Additional Notes:
After having transcribed this presentation, and having added where the share price was as Dr. Mulholland presented the data with each slide
(again, a hearty thanks to this WorldWideTuber YouTube video featuring the share price presented live next to the presentation), one can see the obvious manipulation taking place with the share price to paint the results as if they were poor.
The closing share price from the day before this presentation on May, 9, 2022 was $1.82. The share price opened at $1.71 and without any presentation of the data (Dr. Mulholland had not said a word, and the slide deck had not been posted). When Dr. Mulholland actually began speaking, and when the slide deck was posted on Musella Website, the share price was already at $1.39
So nothing had been made public and the share price had slid by $0.43 per share before the presentation, and before the slide deck had been made public.
Halting the Stock During the Presentation
After seeing the trading share price of the stock as excellent news was released, I’d enquired of the company as to whether they’d anticipated a possible volatile reaction to trading the stock when the presentation had begun.
They told me that they most definitely were concerned about something like this happening. And apparently, and much deliberation, they spent considerable time and effort before Tuesday attempting to get a halt applied to the stock prior to and during the presentation. They mobilized their very reputable OTC and FINRA experts, their legal counsel, and made multiple attempts with the senior levels of FINRA to have a halt enacted, but unfortunately, were unsuccessful in their attempts.